
For women with urge incontinence who fail to respond to medication, more invasive treatments can be offered too, such as botulinum toxin injections (Bladder Botox) into the bladder wall and sacral nerve neuromodulation (SNM).
The flowchart below details surgical options for women with urge incontinence who fail to respond to conservative treatments and medications.
Intra-detrusor Botulinum Toxin Injection (Bladder Botox)
Bladder Botox is effective surgery for women who have urge incontinence that has failed to respond to medications and experience 14 or more episode of urinary leakage a week. This surgery has a success rate of around 85%. Bladder Botox usually wears off over 9 to 12 months and repeat treatments can be performed.
What happens during surgery?
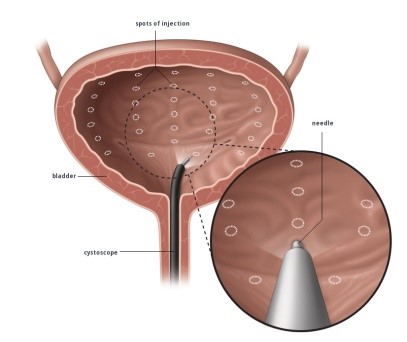
Surgery is performed under direct vision using a cystoscope (a small telescope passed into the bladder through the urethra). Botox is diluted in saline solution an injected into the wall of the bladder at 20 different sites. Surgery takes 10 minutes and can be performed under local anaesthetic, sedation or light general anaesthetic. Usually, you can go home on the day of surgery and return to normal activities after a couple of days.
The illustration below demonstrates the Botox injection into the bladder wall. Surgery is performed under direct vision with patients under local anaesthetic, sedation or light general anaesthetic.
Sacral Neuromodulation (SNM)
SNM may be recommended for women with urge incontinence who fail to respond to conservative treatments and medications. SNM is thought to work by electrically stimulating sacral nerves and nerve centres in the lower spine, which in turn send signals to the nerve centres in brain and restore normal bladder function. Stimulation of sacral nerves is thought to alter bladder sensory pathways and inhibit reflex bladder hyperactivity. SNM is also used to treat some women with urinary retention that is not due to urethral obstruction. Bladder emptying relies ON THE ability of brain pathways to switch-off urethral sphincter guarding reflexes. For women with urinary retention (not due to urethral obstruction) SNM may switch off the excitatory outflow to the urethral sphincter and promote bladder emptying.
Around 75 out of 100 women who have SNM report greater than 50% reduction in urinary leakage and greater than 50% reduction in the number of times they urinate each day. Some women achieve even greater reductions in urinary leakage after SNM surgery.
What happens during surgery?
SNM is performed as a two-stage procedure, under either a light general anaesthetic or sedation with local anaesthetic. During the first stage the sacral lead is placed next to the right or left third sacral nerve root near the middle of the buttock. The lead is connected to a temporary electrical stimulator. Patients leave hospital on the same day as surgery (day surgery) and undergo trial stimulation for a period or one to three weeks (usually one week is sufficient). For patients who experience a positive trial stimulation, the implanted pulse generator (IPG) is connected to the sacral electrode and implanted into the buttock. This surgery is the second stage. Surgery takes only 10 to 15 minutes and patients go home on the same day. Patients have a hand-held unit that allows them to control SNM settings. Training is provided for patients so that they can use the hand-held unit. The IPG unit needs to be changed every 4 to 7 years when it becomes depleted of electrical charge. For women who have a negative trial stimulation, the sacral electrode is removed and other treatment options are considered.
Women who have a SNM system in place are unable to have body MRI scans but can usually have head and limb MRI scans. At airport security, usually a manual security check is required, similar to people who have cardiac pacemakers.
The illustration below demonstrates the sacral electrode placed next to the third sacral nerve root and attached to the implanted pulse generator (IPG). The IPG is implanted in the buttock.

 Dr Carey will be happy to answer any questions you may have and can give more specific advice. Before deciding to have surgery, you should read carefully all the information about your operation and consider obtaining a second opinion.
Dr Carey will be happy to answer any questions you may have and can give more specific advice. Before deciding to have surgery, you should read carefully all the information about your operation and consider obtaining a second opinion.If you experience complications after you leave hospital, contact Dr Carey or the nursing staff on 1 West at the Epworth Freemasons Hospital for advice. In an emergency you may attend the Royal Women’s Hospital, Parkville or Epworth Hospital, Richmond emergency department or attend your closest hospital emergency department.