
Vaginal repair using sutures (mesh free surgery)
Vaginal repair using sutures or stitches to repair the prolapsed vaginal tissues is the commonest form of prolapse surgery. Repairing a prolapse with sutures is often referred to as a colporrhaphy and uses a patient’s own native tissue. No mesh is used in this surgery. This operation is usually recommended for women who have prolapse of the bladder (cystocele) or rectum (rectocele) or a combination of both. This surgery can be performed in combination with other procedures for urinary incontinence and hysterectomy.
What happens during surgery?
Prolapse surgery can be performed with a spinal anaesthetic or a general anaesthetic. Incisions are made inside the vagina and the tissue supporting the vagina is strengthened with stitches. Sutures provide reinforcement of the weakened vaginal tissue. An additional stitch may be required at the top of the vagina or into the cervix to support the vagina or uterus from the sacrospinous ligament. For some women with complex prolapse, surgery may be reinforced with tissue taken through a small incision from the thigh (fascia lata). The vaginal incision is then closed with stitches that will dissolve after two to four weeks. At the end of the operation a catheter is inserted into the bladder to drain urine and a gauze pack is placed in the vagina to prevent bleeding. These will remain in place over night. Antibiotics will be given during the surgery and blood thinning medication is given after surgery.
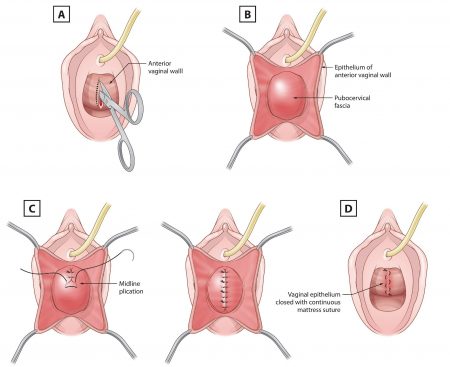
The illustration above demonstrates a vaginal repair of the front wall of the vagina (repair of cystocele). A) An incision is made in the vaginal wall. B) The vaginal wall is separated off the underlying bladder wall. C) The deeper layer is composed of fibrous tissue (pubocervical fascia) and is repaired with stitches. D) The vaginal wall incision is the closed with stitches. A support device is placed into the vagina at the end of end of surgery and is removed 21 to 28 days after surgery in the consulting rooms.
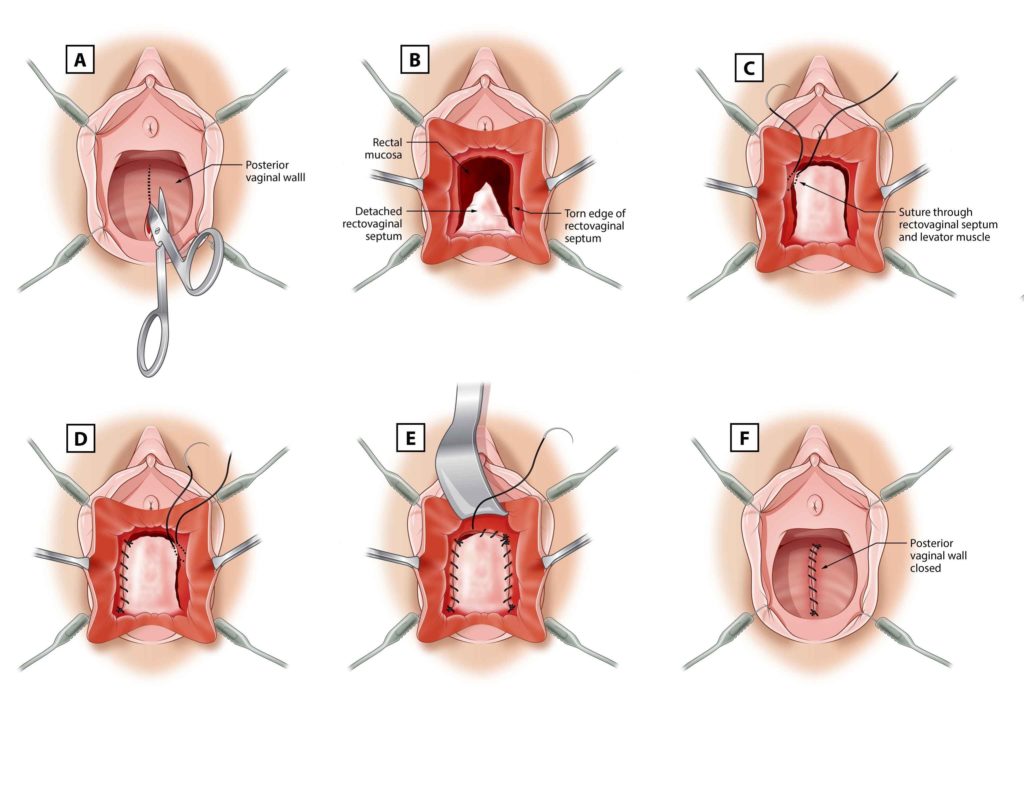 The illustrations above demonstrate a vaginal repair of the back wall of the vagina (repair of rectocele). An incision is made in the vaginal wall. The vaginal wall is separated off the underlying wall of the rectum. The deeper layer is composed of fibrous tissue (rectovaginal fascia) and is repaired with stitches. The vaginal wall incision is closed with stitches.
The illustrations above demonstrate a vaginal repair of the back wall of the vagina (repair of rectocele). An incision is made in the vaginal wall. The vaginal wall is separated off the underlying wall of the rectum. The deeper layer is composed of fibrous tissue (rectovaginal fascia) and is repaired with stitches. The vaginal wall incision is closed with stitches.
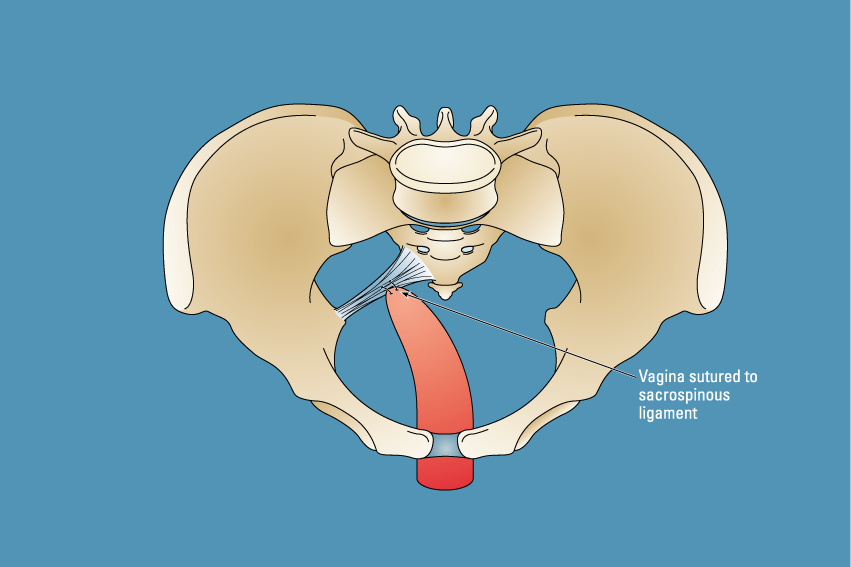
The illustration above demonstrates the sacrospinous fixation operation. The vaginal apex or the uterus is fixed to the sacrospinous ligament providing support of the upper part of the vagina.
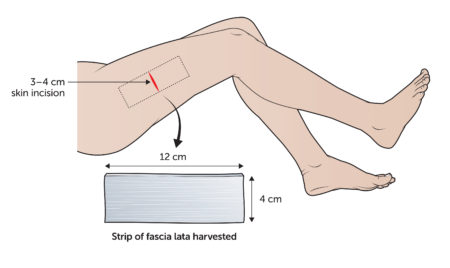
The illustration above shows that fascia lata is taken from a cut in the outer thigh.
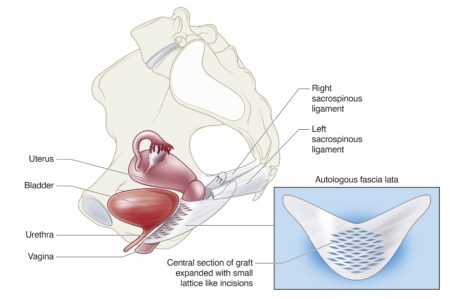
The illustration above shows how fascia lata is used to reinforce an anterior vaginal repair.
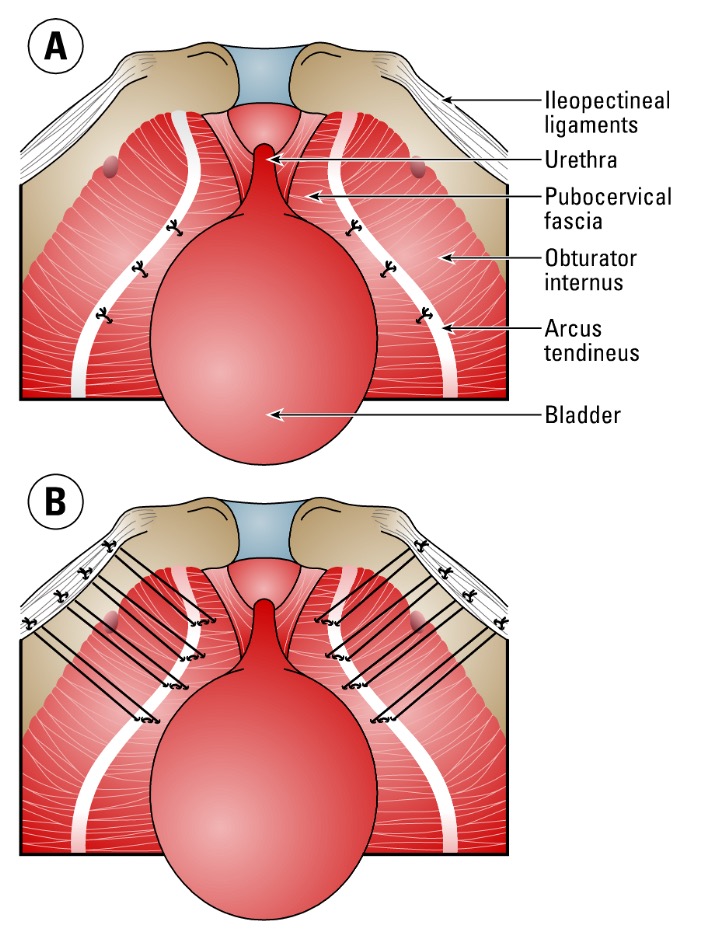
The illustration below shows how: (A) paravaginal repair sutures reattach the front wall of the vaginal to struectures on the sidewall of the pelvis for women who have paravaginal defects; and (B) a Burch colposuspension can be combined with the paravaginal repair to resupport the vagina at the level of the urethra. These two procedures are performed by laparoscopy or robot-assisted laparoscopy.
 Dr Carey will be happy to answer any questions you may have and can give more specific advice. Before deciding to have surgery, you should read carefully all the information about your operation and consider obtaining a second opinion.
Dr Carey will be happy to answer any questions you may have and can give more specific advice. Before deciding to have surgery, you should read carefully all the information about your operation and consider obtaining a second opinion.If you experience complications after you leave hospital, contact Dr Carey or the nursing staff on 1 West at the Epworth Freemasons Hospital for advice. In an emergency you may attend the Royal Women’s Hospital, Parkville or Epworth Hospital, Richmond emergency department or attend your closest hospital emergency department.